
There are 2 types of racism that impact healthcare: institutional racism and personally-mediated racism. The first refers to the “differential
access to goods, services, and opportunities by race” – including access to health insurance and therefore preventive and acute care. The second type refers to individual prejudice or discrimination based on race. Personally-mediated racism can impact the types of treatment options offered to patients and the level of shared decision-making.
Evidence-based practice seeks to guide care decisions through best evidence, physician experience, and patient preferences. To best embody evidence-based practice, physicians should look at racial background in terms of understanding how each patient may be impacted by systemic racism and discrimination. For example, physicians should be aware of historical context, including medical experimentation on slaves and the Tuskegee experiment in the 1900s, in which a group of Black men were unknowingly infected with syphilis by physicians, who observed their symptoms over 40 years without providing any treatment.
These events have led to deep mistrust of physicians within the Black community. In light of this, non-Black physicians should understand these historical impacts and seek to develop good relationships with their patients to build trust. Furthermore, physicians should know about trauma-induced risk factors resulting from stress responses to racial discrimination. These physiological changes can build over time and lead to increased risk of conditions such as cardiovascular disease. Lastly, care providers should work to overcome limitations to access due to lack of insurance coverage. Free options should be presented for testing and other services where patients are not required to have insurance.
When it comes to practice-based evidence, most research focusing on racism in healthcare has used data on patient perceptions of discrimination. These perceptions can have impacts on health, and there has not been much progress in developing accurate methods for assessing physician bias. As long as data on race is captured accurately for patients, quality of care and the services utilized by patients can be analyzed across racial categories. Implicit bias, a major way in which racism impacts quality of care, can be assessed through data collection on the conversations physicians have with patients and what treatments they offer to patients.
So, where does informatics come into the picture?
Informatics plays a huge role in identifying inequities in healthcare practice, as well as collecting data that can be used to understand the causes of these inequities. For example, in order to analyze the quality of care and the services provided to patients across different racial backgrounds, researchers need access to EMR data that has ICD-10 diagnosis codes, CPT codes, and racial data.
Natural language processing (NLP) is a developing area of informatics using machine learning to analyze voice or written conversation data. As voice-driven EMR documentation increases to improve physician user experience, the data collected can be analyzed through NLP to determine attitudes, relationship closeness, and balance of conversation between patients and providers. Coded language terms that indicate bias or discrimination can also be tagged and identified through data mining of the conversation data. This would help to improve the measurement of implicit bias within physicians.
Another approach is to update the standards for social determinants of health to include racism. Based on the potential health impacts of facing discrimination, updating EMRs and other informatics systems to collect patient data on experienced discrimination would help to ensure proper evidence-based practice.
This update to SDOH data could help to improve race-based clinical decision support algorithms that have been criticized for perpetuating system racism through harmful “race-correcting” of outputs. See the chart below from The New England Journal of Medicine for examples of how these algorithms are potentially contributing to disparities in quality of care, rather than mending them.
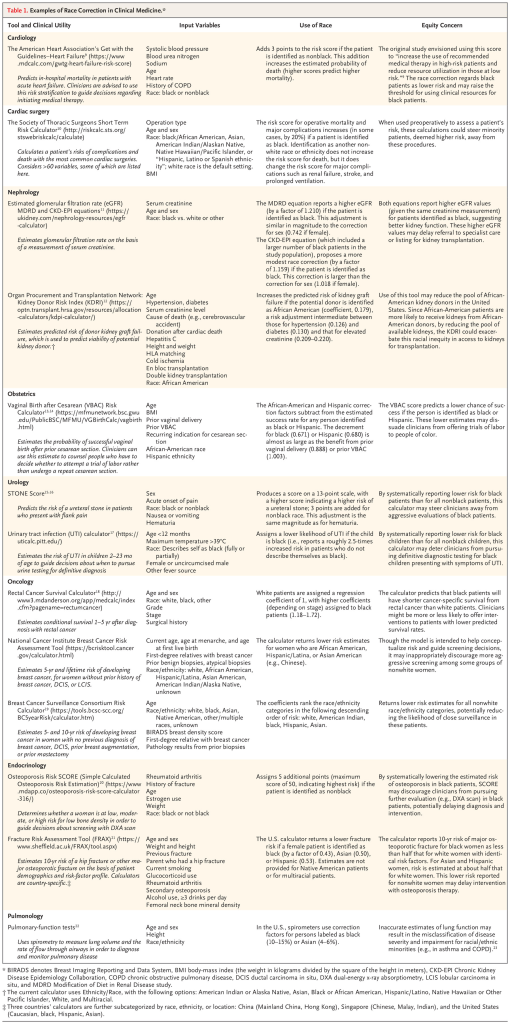
Inaccurately identifying patients as high or low-risk based on race can lead to changes in the services or treatments offered. These algorithms need to be trained to incorporate the nuances of the combined effects of systemic racism and discrimination. As with all informatics research and innovation, sample data used to train any healthcare AI models needs to include equal representation for individuals of all races and demographics to ensure that the technology benefits all demographic groups equally.
References:
Vyas, D. A., M.D., Eisenstein, L. G., M.D., & Jones, D. S., M.D. Ph.D. (2020). Hidden in Plain Sight — Reconsidering the Use of Race Correction in Clinical Algorithms. The New England Journal ofMedicine, (383). https://doi.org/10.1056/NEJMms2004740
